Corner Tumors and Trigeminal Neuralgia
What is a cerebellum? A cerebellum is a specific term referring to the lateral side of the posterior fossa in the brain. The petrous bone, a strong pyramid-shaped bone containing the structures of the inner ear, forms an approximately ninety-degree angle with the cerebellum, a thick membrane called the tentorium (meaning tent in English), which separates the cerebellum from the base of the brain. In this area, located on the lateral edge of the cerebellum, lies the groove between the pons, the egg-shaped, rounded part of the brainstem, and the cerebellum.
This area, where the cerebellum and pons intersect and the petrous bone and tentorium form a corner, contains the 5th cerebral nerve, the 7th and 8th cerebral nerve complexes, and the 9th, 10th, and 11th cerebral nerve complexes. Two important vessels supplying the cerebellum, the AICA and PICA, are also located in this area. The 6th cerebral nerve is also found deep within this area. Thus, when we refer to this corner, we are talking about an extremely complex anatomical region. Tumors, cystic lesions, and various vascular and nerve diseases can occur in this corner region.
The most common lesions located in the corner are:
Corner tumor: vestibular schwannoma 80-90%
Corner meningioma 5-10%
Corner ependymoma
Corner epidermoid cyst
Tumors of the petrous apex
Angular arachnoid cyst
Trigeminal neuralgia
Hemifacial spasm
Glossopharyngeal neuralgia
We use neuromonitoring in facial nerve angle tumor surgeries . We do this to prevent facial paralysis. During the surgery, the neuromonitoring team monitors the facial expressions made by the facial nerve, both audibly and on the screen. However, although neuromonitoring is very useful, it is not always a system that prevents facial paralysis. Despite all precautions, facial paralysis can sometimes develop in facial nerve angle tumors. If facial paralysis develops after facial nerve angle tumor surgery, we wait 3 months, and if there is no improvement, we perform facial resuscitation surgery.

Köşe Tümörü Ameliyatı
Corner Tumor: My male patient, pictured above, had a corner tumor located on the right side. It was quite large, filling the entire corner and compressing half of the brainstem with its cyst. I surgically removed the tumor and its cyst. The pathology report confirmed schwannoma. The patient experienced no neurological regression after surgery. There was no facial paralysis. In fact, his hearing was preserved; he can hear conversations from close range after the surgery, but he cannot understand distant sounds.
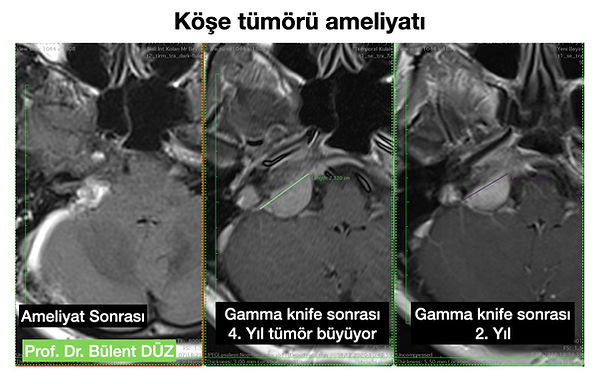

A 42-year-old female patient came to my practice having undergone radiotherapy four years prior for a cranial nerve tumor. She had initially presented with tinnitus. Despite undergoing Gamma Knife treatment over the past four years, the tumor had grown, and she was experiencing balance problems, impaired arm coordination, dizziness, and worsening tinnitus. A cranial nerve tumor becomes more adherent to surrounding tissue after Gamma Knife treatment, making surgery more difficult. Removing a tumor so extensively embedded in the petrous bone at the base of the skull is quite challenging. The greatest risk is facial paralysis. I operated on my patient and removed the tumor almost completely microscopically. The tumor was severely adherent to the facial nerve. I separated the tumor from the nerve and, under neuromonitoring control, removed it without damaging the nerve. After the surgery, my patient was smiling and had no facial paralysis; she left the operating room without experiencing any facial paralysis.